What is sulcus?
Sulcus refers to a crease or invagination of the surface of the vocal fold. It is thought to be caused by a thinning or absence of a special layer of tissue, called the superficial lamina propria, which the vocal cord requires to vibrate in order to produce sound. The lack of this tissue causes a divot in the vocal cord, which gives the disorder its medical name (sulcus means “furrow” in Latin).
The term sulcus encompasses at least two (and possibly more) kinds of lesions. "Sulcus vergeture" is a groove along the entire length of the vocal fold. People with sulcus vergeture typically report a lifetime history of hoarseness, and so many physicians believe it to be a developmental disorder. On rare occasions, sulcus vergeture occurs in families, suggesting that there may be a genetic link.
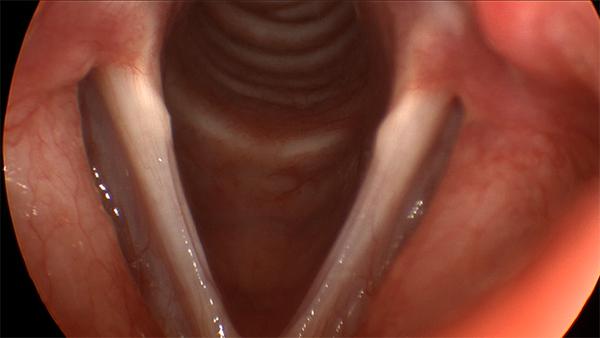
This is the typical appearance of sulcus vergeture. Grooves along the edge of both vocal folds give the appearance of tissue being scooped out.
"Sulcus vocalis", on the other hand, occurs in a limited area of the vocal fold. It is thought to be the consequence of the rupture of a vocal fold cyst, or other scarring process. Unlike sulcus vergeture, associated inflammation often presents itself.
What are the symptoms of sulcus?
Sulcus vergeture causes a characteristic harsh, reedy hoarseness. People with sulcus vergeture frequently must exert unusual effort to produce voice, and find it more difficult to be heard over background noise. Because of the change in pitch which sometimes accompanies this disorder, men with sulcus sometimes complain that they are mistaken for women on the telephone. Sulcus vergeture is usually a lifelong condition, so hoarseness is always present, and the voice is never normal. Most patients cannot recall ever having had a normal voice as an adult, although it is not rare to have had a normal voice as a child.
Sulcus vocalis causes a less specific painless hoarseness. While it may wax and wane, it is typically always present to some degree. Most patients with sulcus vocalis do recall a time when their voice was better.
What does sulcus look like?
Sulcus vergeture has the characteristic appearance of a furrow in the vocal fold, which can vary in depth and location. It is usually found at the margin of the vocal fold, oriented parallel to its length. It usually extends the entire length of the vocal fold. The segment involved with the sulcus usually does not vibrate normally during voicing, an observation that is apparent on stroboscopic examination. When the vocal folds are brought together to voice, the loss of tissue along the length of the folds usually causes a spindle-shaped gap to appear between them. This gap causes air to leak out during voicing, which is likely one of the main reasons for the perception of increased effort needed to voice.
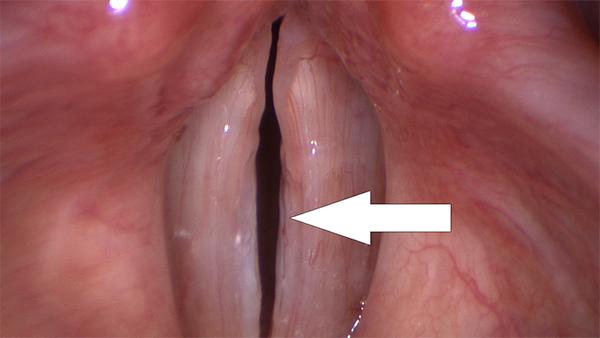
The subtle groove on the edge of the right vocal fold represents a sulcus vocalis.

Both of these vocal folds have a sulcus vocalis - visible as a white line, and more pronounced on the left fold. These sulcus lesions are surrounded by considerable inflammation.
Sulcus vocalis is more localized, and often surrounded by signs of scarring or inflammation, such as rediness and swelling. Like sulcus vergeture, the area of the sulcus does not vibrate normally during voicing, due to the absence of the vibratory layer of the vocal fold.
Typically, sulcus vocalis is subtle and commonly overlooked; the diagnosis is an extremely hard one to make. It is routinely missed by examiners who do not use stroboscopy, because it depends on observing part of the vocal fold not vibrating normally.
How is sulcus treated?
The treatment of sulcus is controversial. The main difficulty involves finding a perfect substitute for the missing superficial lamina propria tissue. Efforts to create a substitute in the laboratory are underway, and may be ready for clinical use in the near future.
Some support the idea that the strip of sulcus should be completely removed, and that neighboring normal tissues should be drawn in to cover the gap left by the removal. While this procedure is sound in theory, it typically results in scarring, with hoarseness that may be equal to or even worse than that caused by sulcus itself.
Other physicians suggest that the vocal fold cover should be lifted up, and a new tissue should be inserted to keep it apart from deeper tissues. Fat from elsewhere in the body, collagen, and other substances are typically used. Results are inconsistent and somewhat unpredictable, but favorable results have been achieved with this method. It is hoped that the development of bioengineered superficial lamina propria tissue, currently being researched, will improve the results obtained with this approach.
Finally, some surgeons, displeased by the unreliability of these first two approaches, settle for injecting the vocal fold to close the spindle-shaped gap created by sulcus. They and their patients accept that this is only a partial solution, but that it may be the best available option.
Those with voice disorders are strongly advised to educate themselves as much as possible regarding their disorder, so that they can make an informed decision regarding treatment. This is especially true in the case of sulcus vocalis, where there is a significant difference of opinion among physicians.