What is a polyp?
A polyp is a specific and clearly demarcated mass (“mass” simply means “lump,” and does not imply cancer or precancerous lesion), usually found at the midpoint of the vocal cord. This typical location suggests that polyps are the result of phonotrauma, the physical stresses on the vocal fold which occur with heavy voice use or voice use under adverse circumstances. Some believe that polyps are formed by localized bleeding, when vocal fold small blood vessels are ruptured by shear forces.
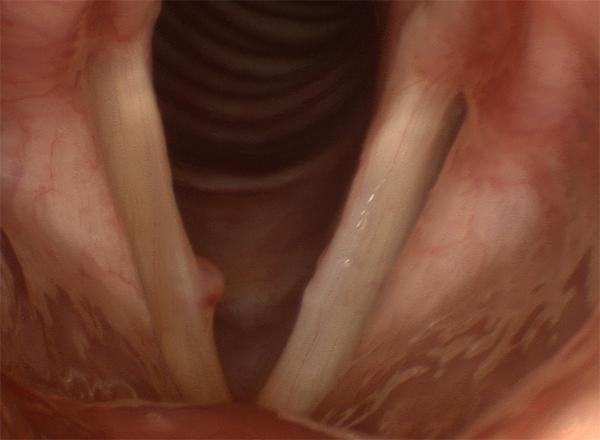
A typical polyp: a red, well-demarcated mid-vocal fold mass
Unlike polyps in other parts of the body, a vocal fold polyp is not a precancerous or cancerous lesion, nor will it ever become one. It should be noted though, that an examination in the office is not always sufficient evidence to distinguish a benign lesion from a malignant one. When the diagnosis is not clear, a biopsy may be necessary.
The term “polyp” is sometimes used generically to refer to any mass of the vocal folds, even by otolaryngologists. In addition to being imprecise, this can lead to confusion and errors in treatment and should be avoided.
What are the symptoms of a polyp?
Polyps generally cause painless hoarseness. The hoarseness results from irregularities in vocal fold closure as well as irregularities in vibration, both the result of the bulk of the polyp. If the polyp has a narrow attachment to the vocal cord, like the neck of a balloon, it may flip in and out of the area of vocal cord closure, and produce only intermittent voice breaks. In some cases, this voice change may be accompanied by the sensation of a foreign body at the level of the vocal folds, or a feeling of wanting to clear the throat.
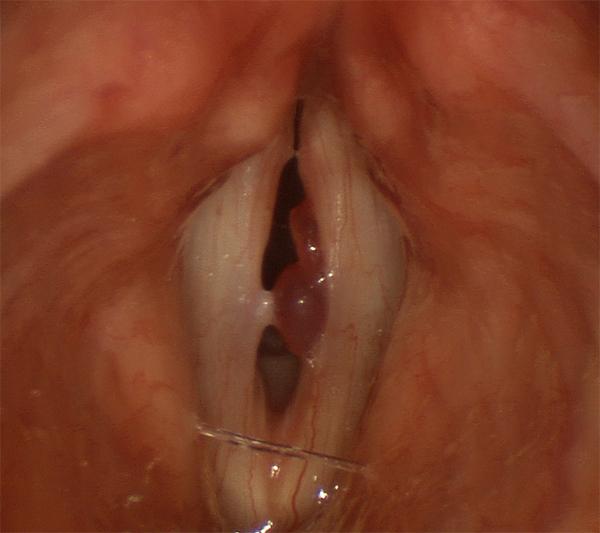
This polyp has two lobes, and interferes with vocal fold closure and vibration during voicing.
What does a polyp look like?
A polyp is usually a red lesion with a sharp margin, and is clearly different from surrounding tissue. It can be either broad-based or narrow-necked. It may be smooth and round, or it may have lobes. Some polyps that have been present for a long time can take on odd shapes, and actual size can vary greatly as well. Polyps usually occur singly, but may also appear in pairs, with one on each vocal fold directly opposite one another. Almost always, they occur at the midpoint of the vocal fold.

A longstanding polyp that has taken an unusual shape
The mid-fold location is so characteristic for a polyp, that a mass occurring elsewhere on the vocal fold should be examined very carefully before settling on a polyp diagnosis.
Polyps do not generally grow over the short-term, although there are exceptions. These exceptions may not represent actual growth, but instead the formation of new polyp tissue from traumatic events, which the initial polyp makes more likely. The propensity for a polyp (or any mid-vocal fold lesion) to cause additional trauma, in addition to their effect on the voice, are factors in favor of their treatment. Any lesion that enlarges rapidly (over weeks) is unlikely to be a polyp and should be considered for removal.
How is a polyp treated?
Voice rest, often prescribed in cases of hoarseness, may improve the voice somewhat but is not likely to make a polyp go away. Voice rest serves to soften and dissolve associated swelling, but the polyp itself is generally too firm and bulky to shrink significantly. People with masses on the vocal fold may find themselves entirely without voice after cheering at a game, or an evening out with friends. Voice rest can help them regain their baseline voice, but the situation will repeat the next time the voice is used strenuously, unless the underlying problem is fixed.
Since a polyp is likely a result of phonotrauma, voice therapy is almost always a good idea - if only to make a patient aware of circumstances and habits of voice use that likely led to the formation of the polyp in the first place. In the case of a small lesion, especially if it has not been present a long time, voice therapy by itself may be enough to minimize the effect of the polyp and restore good voice.
More often than not, polyps require microlaryngoscopic surgery to be removed. Whether an individual should take this step depends on the level of vocal disability, the potential for future damage, and the certainty of the diagnosis. Although there is little evidence to support the use of voice therapy in conjunction with surgery, most laryngologists feel that it is advisable in order to attain the best outcome and reduce the chances of forming another polyp. The chances of forming another polyp after surgery and voice therapy are extremely low.